Blank Cna Shower Sheets Form
The CNA Shower Sheets form plays a crucial role in the daily care of residents in healthcare facilities. This form is designed to facilitate a thorough visual assessment of a resident's skin during showering, ensuring that any abnormalities are promptly identified and addressed. Caregivers, such as Certified Nursing Assistants (CNAs), are responsible for closely examining the skin for issues like bruising, rashes, or lesions. When any irregularities are spotted, the CNA must report these findings to the charge nurse immediately. The form includes a body chart where the CNA can accurately document the location and nature of any skin concerns, which aids in tracking changes over time. Additionally, the form prompts CNAs to assess the need for toenail care, further contributing to the overall well-being of the resident. Following the initial assessment, the charge nurse reviews the findings and provides their own observations, which are also recorded on the form. This collaborative approach ensures that any necessary interventions are communicated to the Director of Nursing (DON) for further evaluation and action. The CNA Shower Sheets form not only enhances communication among the care team but also supports the ongoing monitoring of residents’ skin health, ultimately promoting better patient outcomes.
More PDF Forms
Us Service Animals Esa Letter - This letter is used to validate the presence of an emotional support animal in housing situations.
Alabama Title Application Mvt 20-1 - Review the outline of required information before starting your application.
When purchasing a boat in Arkansas, having a proper Bill of Sale is crucial to confirm the transaction and provide legal protection for both the buyer and the seller. The Bill of Sale for a Boat not only facilitates a smooth transfer of ownership but also ensures that all details pertaining to the sale are documented and clear, preventing any potential disputes in the future.
Employer's Quarterly Federal Tax Return - The IRS 941 form can help identify potential errors in payroll and tax calculations.
Dos and Don'ts
When filling out the CNA Shower Sheets form, it’s essential to ensure accuracy and clarity. Here’s a helpful list of things to do and avoid:
- Do perform a thorough visual assessment of the resident's skin during the shower.
- Do report any abnormalities, such as bruising or rashes, to the charge nurse immediately.
- Do use the body chart to accurately describe and graph all skin abnormalities.
- Do ensure that all required signatures are obtained, including yours and the charge nurse's.
- Do check if the resident needs toenail care and document it appropriately.
- Do forward any issues to the Director of Nursing (DON) for review as needed.
- Do keep a copy of the completed form for your records.
- Don't leave any sections of the form blank; every detail matters.
- Don't use vague descriptions; be specific about any abnormalities observed.
- Don't forget to date the form; it’s important for tracking purposes.
- Don't ignore any signs of skin issues; timely reporting is crucial.
- Don't rush through the assessment; take your time to ensure accuracy.
- Don't alter any information after the form is signed; this can lead to confusion.
- Don't forget to follow up on any concerns raised with the charge nurse.
Cna Shower Sheets Sample
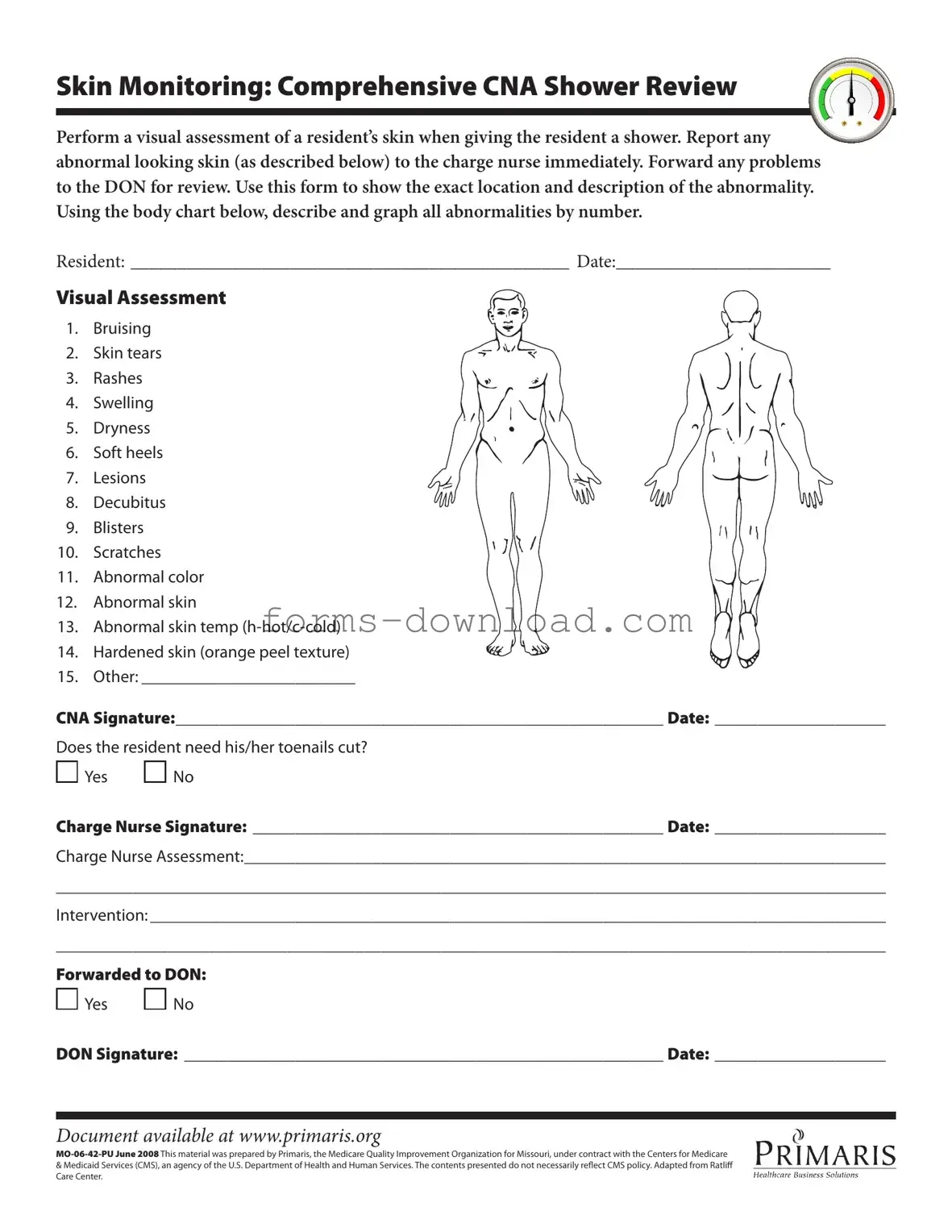
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Listed Questions and Answers
-
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to assist Certified Nursing Assistants (CNAs) in conducting a thorough skin assessment during a resident's shower. It helps document any abnormalities in the resident's skin, ensuring that any issues are reported to the charge nurse promptly for further evaluation and intervention.
-
What types of skin abnormalities should be reported?
During the shower assessment, CNAs should look for a variety of skin abnormalities, including but not limited to bruising, skin tears, rashes, swelling, dryness, soft heels, lesions, decubitus ulcers, blisters, scratches, abnormal color, abnormal skin temperature, and hardened skin. Each of these conditions should be documented accurately on the form.
-
How should abnormalities be documented on the form?
Abnormalities should be documented by using the provided body chart on the form. CNAs should identify the exact location of each abnormality and describe it clearly. This includes numbering the abnormalities on the chart to correspond with the descriptions provided in the list of potential issues.
-
What should a CNA do if they notice an abnormality?
If a CNA observes any abnormal skin condition, they are required to report it immediately to the charge nurse. Following this, the issues should be forwarded to the Director of Nursing (DON) for further review and necessary action.
-
Is there a section for documenting toenail care?
Yes, the form includes a specific section to indicate whether the resident needs their toenails cut. CNAs should check 'Yes' or 'No' as appropriate, ensuring that all aspects of the resident's care are addressed.
-
What happens after the CNA completes the form?
Once the form is completed, it should be signed by the CNA and the charge nurse. The charge nurse will then assess the documented abnormalities and determine the necessary interventions. This information may also be forwarded to the DON for additional oversight.
-
Where can I find this form?
The CNA Shower Sheets form is available online at www.primaris.org. This resource is provided by Primaris, the Medicare Quality Improvement Organization for Missouri, ensuring that CNAs have access to essential documentation tools.
-
Who prepared the CNA Shower Sheets form?
This material was prepared by Primaris under contract with the Centers for Medicare & Medicaid Services (CMS). It is important to note that the contents do not necessarily reflect CMS policy, but they are designed to support quality care in nursing facilities.
Form Overview
| Fact Name | Details |
|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers. |
| Skin Monitoring | CNA staff must perform a visual assessment of the resident’s skin and report any abnormalities to the charge nurse immediately. |
| Abnormalities List | The form includes a list of potential skin issues such as bruising, skin tears, rashes, and decubitus. |
| Signature Requirements | Both the CNA and the charge nurse must sign the form, indicating their assessments and actions taken. |
| Forwarding Issues | Any identified problems must be forwarded to the Director of Nursing (DON) for further review. |
| Governing Law | This form is governed by regulations under the Centers for Medicare & Medicaid Services (CMS). |