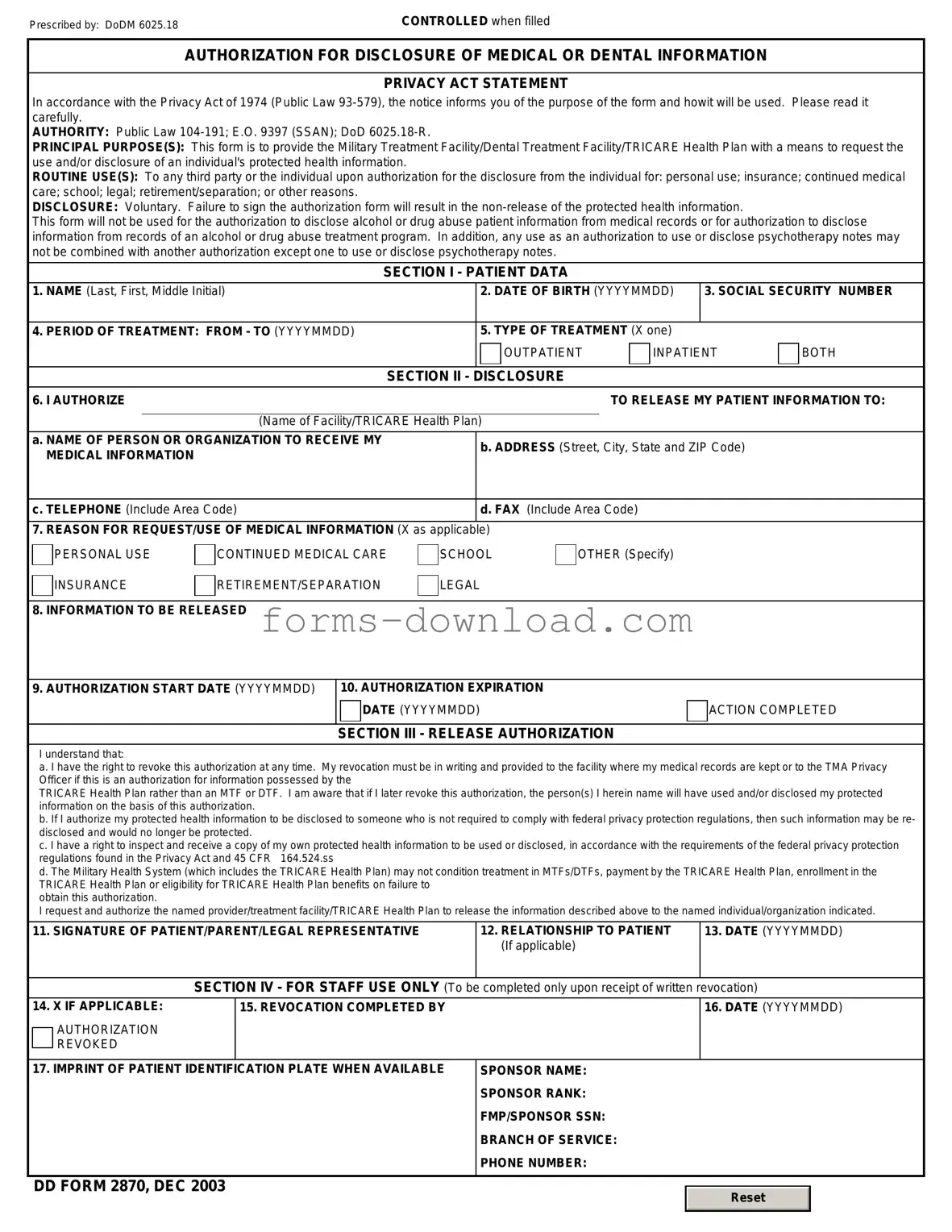
Blank DD 2870 Form
The DD 2870 form plays a crucial role in the realm of military health care, serving as a vital document for individuals seeking to authorize the release of their medical information. This form is particularly important for service members, veterans, and their dependents, as it ensures that pertinent health records can be shared with authorized entities, such as healthcare providers or insurance companies. By allowing the disclosure of medical records, the DD 2870 facilitates continuity of care and ensures that individuals receive the necessary medical attention, especially when transitioning between different healthcare systems. It is essential for users to understand the specific sections of the form, which require detailed information about the patient, the type of information to be released, and the duration of the authorization. Additionally, the DD 2870 emphasizes the importance of informed consent, underscoring the need for individuals to be aware of their rights regarding their medical information. As a tool designed to protect patient privacy while allowing for necessary communication, the DD 2870 form is integral to the effective functioning of military healthcare services.
More PDF Forms
Therapy Progress Note - Notes on any emergencies encountered during the visit.
Dd 214 - The form serves as an official record of military education completed during service.
The Missouri Boat Bill of Sale form is essential for anyone looking to buy or sell a boat in the state of Missouri. This document not only simplifies the transfer of ownership but also provides legal protection for both parties involved in the transaction. To ensure that all necessary information is documented accurately, you can use the Bill of Sale for a Boat, which is designed to help you navigate the process with ease.
High School Transcript - Contains course names, credits earned, and a summary of academic standing.
Dos and Don'ts
When filling out the DD 2870 form, it's important to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn't do:
- Do read the instructions carefully before starting the form.
- Do provide accurate and complete information.
- Do use black or blue ink for legibility.
- Do double-check your entries for any errors.
- Do sign and date the form where required.
- Don't leave any required fields blank.
- Don't use white-out or correction fluid on the form.
- Don't submit the form without making a copy for your records.
- Don't forget to check for additional documents that may be required.
DD 2870 Sample
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Listed Questions and Answers
-
What is the DD 2870 form?
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is a document used by the Department of Defense. It allows military personnel and their dependents to authorize the release of their medical or dental records to specified individuals or entities. This form is essential for ensuring that health information is shared appropriately, especially when seeking treatment or transferring care.
-
Who needs to fill out the DD 2870 form?
Any active duty service member, reservist, or dependent who requires their medical or dental records to be shared with another healthcare provider or institution should complete the DD 2870 form. This includes situations where a patient is moving to a new location, changing doctors, or needing to provide records for legal purposes.
-
How do I complete the DD 2870 form?
To complete the DD 2870 form, follow these steps:
- Begin by providing your personal information, including your name, Social Security number, and contact details.
- Indicate the specific medical or dental information you wish to disclose.
- Clearly state the purpose of the disclosure, whether it is for treatment, legal matters, or another reason.
- Designate the individual or organization to whom the information will be sent.
- Sign and date the form to authorize the release of your records.
It is crucial to review the completed form for accuracy before submission to avoid any delays in processing your request.
-
Where do I submit the DD 2870 form?
The submission process for the DD 2870 form depends on the specific circumstances surrounding the request. Generally, you should submit the completed form to the healthcare facility or provider that holds your medical or dental records. If you are unsure where to send it, contacting the facility directly can provide clarity. Additionally, some military installations may have specific instructions or online portals for submitting such requests.
Form Overview
| Fact Name | Description |
|---|---|
| Purpose | The DD Form 2870 is used to request access to military medical records. |
| Who Uses It | Service members, veterans, and authorized representatives utilize this form. |
| Submission Method | The form can be submitted in person, by mail, or electronically, depending on the facility. |
| Required Information | Personal identification details, such as name, Social Security number, and contact information, are required. |
| Privacy Act Compliance | The form complies with the Privacy Act of 1974, ensuring personal information is protected. |
| Processing Time | Processing times can vary, but requests are typically handled within 30 days. |
| State-Specific Laws | Each state may have additional laws regarding medical records access; check local regulations. |
| Fees | Generally, there are no fees for accessing military medical records using this form. |
| Form Updates | The DD Form 2870 may be updated periodically; always use the latest version available. |
| Contact Information | For assistance, contact the military medical facility or the appropriate records office. |