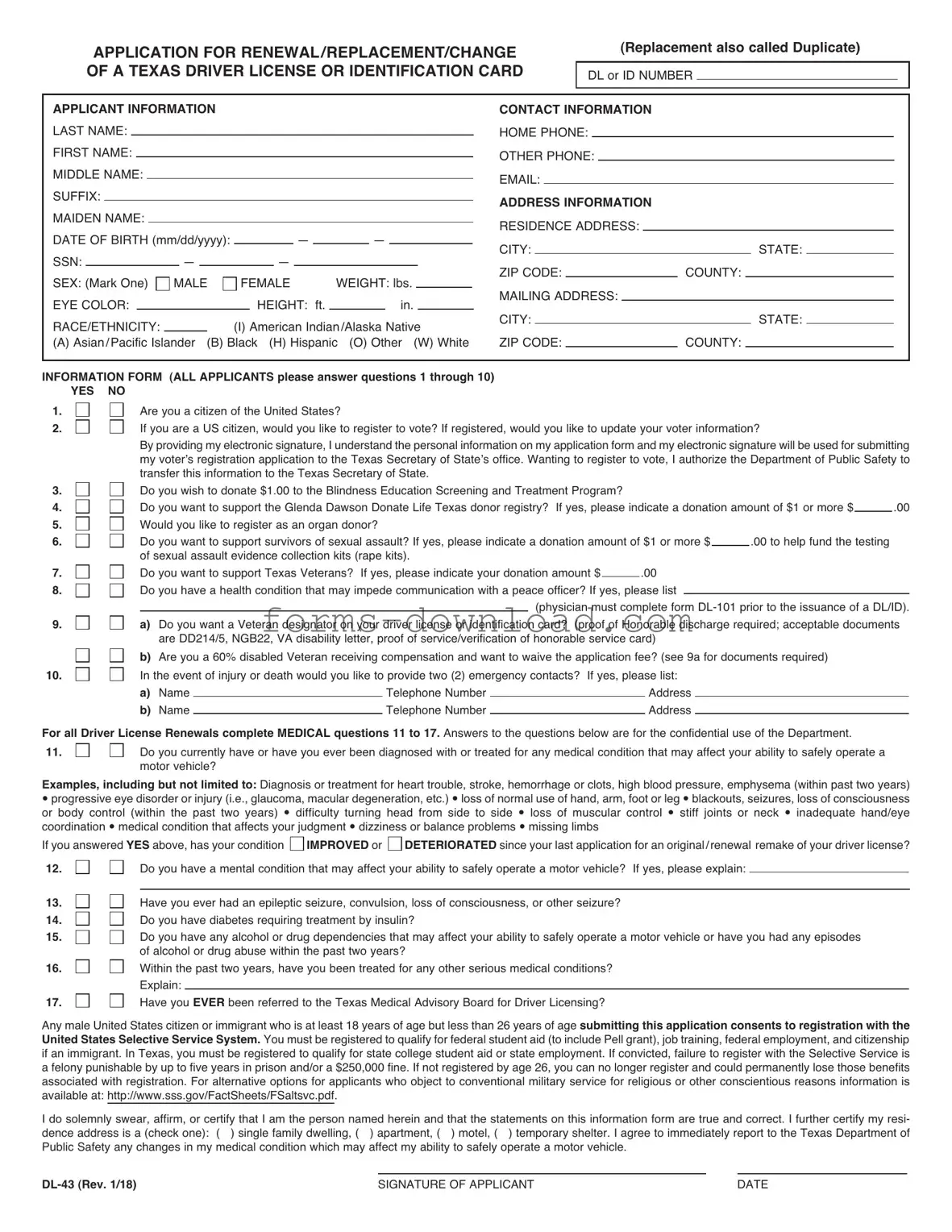
Blank DL-43 Form
The DL-43 form plays a crucial role in the realm of driver's licensing and identification in the United States. This document is primarily utilized by individuals seeking to obtain or renew a driver's license or state-issued identification card. It serves as an official application that collects essential personal information, including the applicant's name, address, date of birth, and Social Security number. Additionally, the DL-43 form may require details about previous licenses held, any medical conditions that could affect driving ability, and the applicant's signature, which affirms the accuracy of the provided information. Understanding the requirements and implications of the DL-43 form is vital for anyone navigating the licensing process. Failure to complete the form accurately can lead to delays or denials, emphasizing the importance of careful attention to detail. Moreover, the form often includes instructions for submitting supporting documents, such as proof of residency or identity, which are necessary to validate the application. Overall, the DL-43 form is a fundamental component of ensuring that individuals meet the legal criteria for driving and identification, thereby contributing to public safety and regulatory compliance.
More PDF Forms
CBP Form 6059B - Each traveler, including children, must submit a CBP 6059B.
For those embarking on the journey of homeschooling, utilizing a detailed Homeschool Letter of Intent preparation guide can be immensely beneficial. This form not only signifies your commitment to home education but also ensures that you meet all necessary state requirements.
Make Your Own Gift Certificate - Support local businesses with a gift certificate purchase.
Dos and Don'ts
When filling out the DL-43 form, it's important to follow certain guidelines to ensure everything goes smoothly. Here’s a helpful list of dos and don'ts:
- Do read the instructions carefully before starting.
- Do use black or blue ink to fill out the form.
- Do double-check all your information for accuracy.
- Do sign and date the form where required.
- Do keep a copy of the completed form for your records.
- Don't leave any required fields blank.
- Don't use white-out or correction fluid on the form.
- Don't submit the form without all necessary documents attached.
- Don't forget to check the expiration date of your ID.
- Don't rush through the process; take your time to ensure everything is correct.
DL-43 Sample
|
APPLICATION FOR RENEWAL/REPLACEMENT/CHANGE |
|
|
|
|
|
|
(Replacement also called Duplicate) |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||
|
OF A TEXAS DRIVER LICENSE OR IDENTIFICATION CARD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
DL or ID NUMBER |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICANT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTACT INFORMATION |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
LAST NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME PHONE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
FIRST NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER PHONE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
MIDDLE NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMAIL: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
SUFFIX: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS INFORMATION |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
MAIDEN NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RESIDENCE ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
DATE OF BIRTH (mm/dd/yyyy): |
|
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
|
|
CITY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE: |
|
|
|
|
|
|||||||||||||||||||
SSN: |
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ZIP CODE: |
|
|
|
|
|
|
|
|
COUNTY: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||
SEX: (Mark One) |
|
MALE |
|
FEMALE |
|
|
WEIGHT: lbs. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
MAILING ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
EYE COLOR: |
|
|
|
|
|
|
|
|
|
|
|
|
|
HEIGHT: ft. |
|
|
|
|
|
|
in. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
RACE/ETHNICITY: |
|
|
|
|
|
|
|
(I) |
American Indian/Alaska |
Native |
|
|
CITY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE: |
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
(A) Asian/Pacific Islander |
(B) Black (H) Hispanic (O) Other |
(W) White |
ZIP CODE: |
|
|
|
|
|
|
|
|
COUNTY: |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMATION FORM (ALL APPLICANTS please answer questions 1 through 10) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
1. YES NO |
|
Are you a citizen of the United States? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
2. |
|
|
|
|
|
If you are a US citizen, would you like to register to vote? If registered, would you like to update your voter information? |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
By providing my electronic signature, I understand the personal information on my application form and my electronic signature will be used for submitting |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
my voter’s registration application to the Texas Secretary of State’s office. Wanting to register to vote, I authorize the Department of Public Safety to |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
3. |
|
|
|
|
|
transfer this information to the Texas Secretary of State. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
Do you wish to donate $1.00 to the Blindness Education Screening and Treatment Program? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
4. |
|
|
|
|
|
Do you want to support the Glenda Dawson Donate Life Texas donor registry? If yes, please indicate a donation amount of $1 or more $ |
|
.00 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
5. |
|
|
|
|
|
Would you like to register as an organ donor? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
6. |
|
|
|
|
|
Do you want to support survivors of sexual assault? If yes, please indicate a donation amount of $1 or more $ |
|
|
|
.00 to help fund the testing |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
7. |
|
|
|
|
|
of sexual assault evidence collection kits (rape kits). |
|
|
|
|
|
|
|
|
|
.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
Do you want to support Texas Veterans? |
If yes, please indicate your donation amount $ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
8. |
|
|
|
|
|
Do you have a health condition that may impede communication with a peace officer? If yes, please list |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
9. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(physician must complete form |
||||||||||||||||||||||||
|
|
|
|
|
a) Do you want a Veteran designator on your driver license or identification card? |
(proof of Honorable discharge required; acceptable documents |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
b) |
are DD214/5, NGB22, VA disability letter, proof of service/verification of honorable service card) |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
10. |
|
|
|
|
|
Are you a 60% disabled Veteran receiving compensation and want to waive the application fee? (see 9a for documents required) |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
In the event of injury or death would you like to provide two (2) emergency contacts? If yes, please list: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
a) |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
b) |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
For all Driver License Renewals complete MEDICAL questions 11 to 17. Answers to the questions below are for the confidential use of the Department. |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
11. |
|
|
|
|
|
Do you currently have or have you ever been diagnosed with or treated for any medical condition that may affect your ability to safely operate a |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
motor vehicle? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Examples, including but not limited to: Diagnosis or treatment for heart trouble, stroke, hemorrhage or clots, high blood pressure, emphysema (within past two years) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
progressive eye disorder or injury (i.e., glaucoma, macular degeneration, etc.) loss of normal use of hand, arm, foot or leg blackouts, seizures, loss of consciousness |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
or body control (within the past two years) |
difficulty turning head from side to side |
loss of muscular control stiff joints or neck inadequate hand/eye |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
coordination medical condition that affects your judgment dizziness or balance problems |
missing limbs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
If you answered YES above, has your condition |
IMPROVED or |
DETERIORATED since your last application for an original/renewal remake of your driver license? |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
12. |
|
|
|
|
|
Do you have a mental condition that may affect your ability to safely operate a motor vehicle? |
If yes, please explain: |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
13. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Have you ever had an epileptic seizure, convulsion, loss of consciousness, or other seizure? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
14. |
|
|
|
|
Do you have diabetes requiring treatment by insulin? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
15. |
|
|
|
|
Do you have any alcohol or drug dependencies that may affect your ability to safely operate a motor vehicle or have you had any episodes |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||
16. |
|
|
|
|
of alcohol or drug abuse within the past two years? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
Within the past two years, have you been treated for any other serious medical conditions? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
17. |
|
|
|
|
Explain: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
Have you EVER been referred to the Texas Medical Advisory Board for Driver Licensing? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
Any male United States citizen or immigrant who is at least 18 years of age but less than 26 years of age submitting this application consents to registration with the |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
United States Selective Service System. You must be registered to qualify for federal student aid (to include Pell grant), job training, federal employment, and citizenship |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
if an immigrant. In Texas, you must be registered to qualify for state college student aid or state employment. If convicted, failure to register with the Selective Service is |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
a felony punishable by up to five years in prison and/or a $250,000 fine. If not registered by age 26, you can no longer register and could permanently lose those benefits |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
associated with registration. For alternative options for applicants who object to conventional military service for religious or other conscientious reasons information is |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
available at: http://www.sss.gov/FactSheets/FSaltsvc.pdf. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
I do solemnly swear, affirm, or certify that I am the person named herein and that the statements on this information form are true and correct. I further certify my resi- |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
dence address is a (check one): ( |
) single family dwelling, ( |
|
) apartment, ( ) motel, ( |
) temporary shelter. I agree to immediately report to the Texas Department of |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Public Safety any changes in my medical condition which may affect my ability to safely operate a motor vehicle. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF APPLICANT |
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
||||||||||||||||||||||||||||||
|
SOLICITUD PARA RENOVAR, REEMPLAZAR, Ó HACER |
|
(El reemplazo también es llamado duplicado) |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
CAMBIOS EN LA LICENCIA DE CONDUCIR O TARJETA DE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
NUMERO DE LICENCIA O DE TARJETA DE IDENTIFICACIÓN: |
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
IDENTIFICACIÓN DEL ESTADO DE TEXAS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMACIÓN DEL SOLICITANTE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMACIÓN DE CONTACTO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
APELLIDO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NÚMERO DE TELÉFONO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
PRIMER NOMBRE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELÉFONO SECUNDARIO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
SEGUNDO NOMBRE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CORREO ELECTRÓNICO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
SUFIJO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SU DOMICILIO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
APELLIDO DE SOLTERA: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOMICILIO DONDE RESIDE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
FECHA DE NACIMIENTO (mm/dd/aaaa): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CIUDAD: |
|
|
|
|
|
|
|
|
|
|
|
|
|
ESTADO: |
|
|
|
|
|
||||||||||||||||
NÚMERO DE SEGURO SOCIAL: |
|
|
|
|
|
— |
|
|
— |
|
|
|
|
|
|
|
|
|
|
CÓDIGO POSTAL: |
|
|
|
|
CONDADO: |
|
|
|
|
|
|
||||||||||||||||||||||
SEXO: (Marque uno) |
HOMBRE |
MUJER |
PESO: en libres. |
|
|
|
|
|
|
DOMICILIO POSTAL (Lugar donde recibe su correspondencia): |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
COLOR DE LOS OJOS: |
|
|
|
|
|
|
|
|
ESTATURA: pies |
|
|
|
|
pulg. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
RAZA/ETNIA: |
|
|
|
(I) Amerindio/Nativo de Alaska |
(A) Asiático/nativo |
|
|
|
CIUDAD: |
|
|
|
|
|
|
|
|
|
|
|
ESTADO: |
|
|
|
|
|
|||||||||||||||||||||||||||
de las Islas del Pacífico (B) Negro (H) Hispano (O) Otro (W) Blanco |
|
|
|
|
|
|
CÓDIGO POSTAL: |
|
|
|
|
CONDADO: |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
INFORMACIÓN SOBRE EL SOLICITANTE (TODOS LOS SOLICITANTES favor de contestar las preguntas 1 a 10) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
1. |
SI NO |
¿Es usted ciudadano de los Estados Unidos? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
2. |
|
|
|
Si usted es ciudadano de los Estados Unidos, ¿le gustaría registrarse para votar? Si ya está registrado, ¿le gustaría actualizar su información de votante? |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
Al proporcionar mi firma electrónica, comprendo que la información personal en mi solicitud, junto con mi firma electrónica, se usará para enviar mi |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
solicitud de registro electoral a la oficina de la Secretaría del Estado de Texas. Deseo registrarme para votar; por lo tanto, autorizo al Departamento |
|||||||||||||||||||||||||||||||||||||||||||||||||
3. |
|
|
|
de Seguridad Pública para transferir esta información a la Secretaría del Estado de Texas. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
¿Desea usted donar $1.00 al Programa de Educación, Evaluación y Tratamiento de la Ceguera? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
4. |
|
|
|
¿Desea apoyar el Programa de Registro de |
|||||||||||||||||||||||||||||||||||||||||||||||||
5. |
|
|
|
de $1 o más $ |
.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
¿Desea registrarse como donador de órganos? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
6. |
|
|
|
¿Quieres apoyar a los sobrevivientes de asalto sexual? Si es así, porfavor indique la cantidad de donación de $1 o más $ |
|
|
.00 para |
||||||||||||||||||||||||||||||||||||||||||||||
7. |
|
|
|
ayudar a financiar la recopilación de evidencia de asalto sexual (kit de violación) |
|
|
|
|
|
|
.00 |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
¿Desea apoyar los Veteranos de Texas? Si la respuesta es sí, por favor, indique la cantidad de su donación $ |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
8. |
|
|
|
¿Tiene usted alguna afección médica que le pueda impedir la comunicación con un oficial de la policía? En caso afirmativo, por favor indique |
|||||||||||||||||||||||||||||||||||||||||||||||||
9. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(el médico debe llenar el formulario |
||||||||||||||||||||||||||||||||||||
|
|
|
a) Desea una insignia de Veterano en su licencia de conducir o su tarjeta de identificación? (Se requiere comprobante de baja honorable; los |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
b) |
documentos aceptables son DD214/5, NGB22, carta de discapacidad del VA, prueba de servicio/verificación de la tarjeta de servicio honorable) |
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
¿Es usted un Veterano que recibe 60% de compensación por discapacidad y desea quedar exento de los derechos de solicitud? |
|||||||||||||||||||||||||||||||||||||||||||||||||
10. |
|
|
|
|
(vea el punto 9a para conocer qué documentos se requieren). |
|
|
|
|
|
|
|
|
En caso afirmativo, por favor indique: |
|||||||||||||||||||||||||||||||||||||||
|
|
|
En caso de sufrir lesiones o la muerte, ¿le gustaría proporcionar dos (2) contactos para emergencias? |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
a) |
Nombre |
|
|
|
|
|
|
|
|
|
|
|
|
|
Número telefónico |
|
|
|
|
|
|
|
|
|
Domicilio |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
b) |
Nombre |
|
|
|
|
|
|
|
|
|
|
|
|
|
Número telefónico |
|
|
|
|
|
|
|
|
|
Domicilio |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Para todas las Renovaciones de Licencia de Conducir, complete las preguntas MÉDICAS 11 a 17. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
Las respuestas a las siguientes preguntas son para uso confidencial del Departamento. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
11. |
|
|
|
¿Tiene actualmente o alguna vez ha sido diagnosticado con o tratado por alguna enfermedad que pueda afectar su capacidad de |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
operar un vehículo motorizado de manera segura? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
Ejemplos, incluyendo pero no limitado a: Diagnóstico o tratamiento por problemas cardíacos, derrame cerebral, hemorragia o coágulos, presión arterial alta, enfisema (en los últi- |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
mos dos años) enfermedad progresiva o lesión de la vista (como glaucoma, degeneración macular, etc.) pérdida del uso normal de la mano, brazo, pie o pierna desvanec- |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
imientos, ataques, pérdida de la consciencia o control del cuerpo (en los últimos dos años) |
dificultad para voltear la cabeza de un lado a otro |
pérdida de control muscular artic- |
|||||||||||||||||||||||||||||||||||||||||||||||||||
ulaciones o cuello rígidos coordinación inadecuada de mano/ojo afección médica que altere su juicio mareos o problemas de equilibrio pérdida de algún miembro |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
Si respondió SÍ a la pregunta anterior, ¿su afección ha |
MEJORADO o |
EMPEORADO desde su última solicitud de original/renovación de licencia de conducir? |
|||||||||||||||||||||||||||||||||||||||||||||||||||
12. |
|
|
|
¿Tiene usted un condición mental que puede afectar su capacidad para operar con seguridad un vehículo motorizado? Si su respuesta es si, |
|||||||||||||||||||||||||||||||||||||||||||||||||
13. |
|
|
|
por favor de explicar: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
¿Alguna vez ha tenido un ataque epiléptico, convulsión, pérdida de la consciencia u otro ataque? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
14. |
|
|
|
¿Tiene diabetes que requiera tratamiento con insulina? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
15. |
|
|
|
¿Tiene alguna dependencia del alcohol o de drogas que pudiera afectar su capacidad de operar un vehículo motorizado de manera |
|||||||||||||||||||||||||||||||||||||||||||||||||
16. |
|
|
|
segura o ha tenido algún episodio de abuso de drogas o alcohol en los últimos dos años? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
En los últimos dos años, ¿ha recibido tratamiento por alguna otra afección médica grave? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
17. |
|
|
|
Explique: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
¿Alguna vez ha sido remitido al Comité Asesor Médico de Licencias de Conducir de Texas? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
Cualquier hombre ciudadano o inmigrante de los Estados Unidos entre 18 y 26 años de edad que presente esta solicitud otorga su consentimiento para ser registrado |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
en el Sistema de Servicio Militar Selectivo de los Estados Unidos. Usted debe estar registrado para tener derecho a recibir ayuda federal estudiantil (incluso la beca |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
Pell Grant), capacitación laboral, empleo federal y la ciudadanía si es inmigrante,. En Texas, usted debe estar registrado para tener derecho a recibir ayuda estudiantil |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
universitaria o empleo con el Estado. No registrarse en el Servicio Militar Selectivo es un delito mayor. Si es declarado culpable de ello, podría ser castigado hasta con |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
cinco años de prisión y/o una multa de 250,000 dólares. Si no se ha registrado antes de cumplir 26 años, ya no se podrá registrar y podría perder permanentemente los |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
beneficios asociados con el registro. Para conocer otras opciones alternativas para solicitantes que se oponen al servicio militar convencional por motivos religiosos u otros |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
motivos de conciencia, podrá encontrar información disponible en: http://www.sss.gov/FactSheets/FSaltsvc.pdf. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
Juro solemnemente, afirmo o certifico que soy la persona que se indica en el presente documento y que las declaraciones en esta solicitud son verdaderas y correctas. Además |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
certifico que mi domicilio de residencia es (marque una opción): ( |
) casa residencial, ( |
|
) apartamento, ( ) hotel, ( ) sitio de refugio temporal. Estoy de acuerdo en informar |
||||||||||||||||||||||||||||||||||||||||||||||||||
inmediatamente al Departamento de Seguridad Pública de Texas cualquier cambio en mi condición médica que pueda afectar mi capacidad para conducir de manera segura |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
un vehículo motorizado. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FIRMA DEL ASPIRANTE |
|
|
|
|
|
|
|
|
|
|
|
|
|
FECHA |
|
|
|
|
|||||||||||||||||
Listed Questions and Answers
-
What is the DL-43 form?
The DL-43 form is a specific application used in the United States for requesting a duplicate or replacement driver's license. It is typically utilized when a driver has lost their license, had it stolen, or needs to update personal information.
-
Who needs to fill out the DL-43 form?
Any individual who holds a driver's license in the state and requires a duplicate or replacement should complete the DL-43 form. This includes anyone who has experienced loss, theft, or changes in personal details such as name or address.
-
Where can I obtain the DL-43 form?
The DL-43 form can usually be obtained from your state’s Department of Motor Vehicles (DMV) website or office. Many states also provide the option to fill it out online, making the process more convenient.
-
What information do I need to provide on the DL-43 form?
When completing the DL-43 form, you will typically need to provide personal information such as your full name, date of birth, address, and driver's license number. Additionally, you may need to indicate the reason for requesting a duplicate or replacement.
-
Is there a fee associated with the DL-43 form?
Yes, there is usually a fee for processing the DL-43 form. The amount can vary by state, so it’s best to check your local DMV’s website for the exact fee and payment methods accepted.
-
How long does it take to receive my new license after submitting the DL-43 form?
The processing time for receiving your new driver's license can vary. In many cases, you may receive it within a few weeks, but it could take longer depending on your state’s processing times and workload.
-
Can I submit the DL-43 form online?
Many states allow you to submit the DL-43 form online, which can expedite the process. However, some states may require you to visit a DMV office in person, especially if you are updating personal information.
-
What should I do if my DL-43 form is denied?
If your application is denied, you should receive a notification explaining the reason. Common issues include missing information or failure to provide proper identification. You can often resolve these issues by providing the required documentation or correcting any mistakes.
-
Can I track the status of my DL-43 application?
Many states provide a way to track the status of your DL-43 application online. Check your state’s DMV website for specific instructions on how to monitor your application’s progress.
Form Overview
| Fact Name | Details |
|---|---|
| Purpose | The DL-43 form is primarily used for applying for a driver's license in certain states. |
| Governing Law | In Pennsylvania, the DL-43 form is governed by Title 75 of the Pennsylvania Consolidated Statutes. |
| Eligibility | Applicants must meet specific age and residency requirements to use the DL-43 form. |
| Identification Requirements | Individuals must provide proof of identity, residency, and Social Security number when submitting the form. |
| Submission Method | The DL-43 form can typically be submitted online, by mail, or in person at designated locations. |
| Processing Time | Processing times for the DL-43 form may vary, but applicants often receive their licenses within a few weeks. |
| Fees | There is usually a fee associated with the application process, which varies by state. |
| Renewal | The DL-43 form is also used for renewing a driver's license, subject to certain conditions. |
| Additional Resources | State-specific DMV websites provide additional information and resources related to the DL-43 form. |