Blank Employment verification form Form
When it comes to the hiring process, employers often need to confirm a candidate's work history and qualifications. The Employment Verification Form serves as a crucial tool in this process. This form is typically used by employers to gather essential information about a potential employee's previous jobs, including dates of employment, job titles, and responsibilities. It may also request details about the employee's performance and conduct while employed. By completing this form, previous employers can provide valuable insights that help hiring managers make informed decisions. Additionally, the form ensures that the verification process remains consistent and organized, making it easier for all parties involved. Understanding the importance and components of the Employment Verification Form can streamline the hiring process and promote transparency between employers and candidates.
More PDF Forms
Can a Dishonorable Discharge Be Reversed - Filing a DD 149 can take several months for processing and review.
When purchasing a vehicle, it is crucial to understand the importance of utilizing the proper documentation. A reliable resource for navigating the transaction is a thorough guide on how to complete the essential components of your bill of sale form, which can be found at effective bill of sale form documentation.
Australian Passport Renewal Form - Renew your passport well ahead of any planned travel to avoid last-minute complications.
Dos and Don'ts
When filling out an employment verification form, it is essential to approach the task with care and attention to detail. Here are ten important guidelines to follow, including things you should do and things to avoid.
- Do read the entire form before starting to fill it out.
- Do provide accurate and up-to-date information about your employment history.
- Do include all relevant details, such as job titles, dates of employment, and responsibilities.
- Do double-check your entries for any typographical errors.
- Do sign and date the form where required.
- Don't leave any sections blank unless instructed to do so.
- Don't provide false or misleading information; this can have serious consequences.
- Don't rush through the process; take your time to ensure accuracy.
- Don't forget to include contact information for your previous employers if required.
- Don't ignore any specific instructions provided with the form.
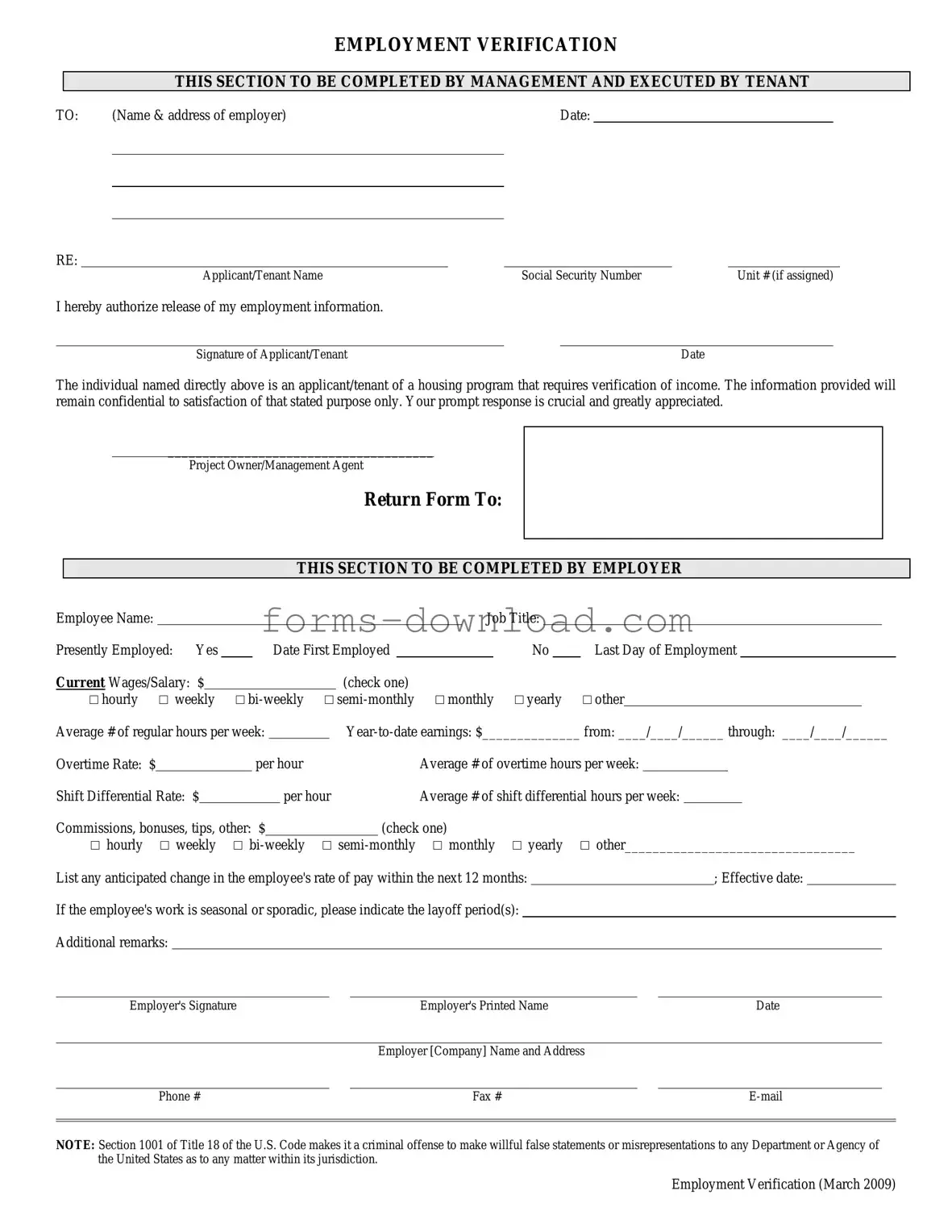
Employment verification form Sample
EMPLOYMENT VERIFICATION
THIS SECTION TO BE COMPLETED BY MANAGEMENT AND EXECUTED BY TENANT
TO: |
(Name & address of employer) |
Date: |
|
|
|
|
|
|
|
|
|
RE:
Applicant/Tenant Name |
|
Social Security Number |
|
Unit # (if assigned) |
I hereby authorize release of my employment information.
Signature of Applicant/Tenant |
|
Date |
The individual named directly above is an applicant/tenant of a housing program that requires verification of income. The information provided will remain confidential to satisfaction of that stated purpose only. Your prompt response is crucial and greatly appreciated.
______________________________________
Project Owner/Management Agent
Return Form To:
THIS SECTION TO BE COMPLETED BY EMPLOYER
Employee Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Job Title: |
|
|
|
|
|
|
|
|
||||
Presently Employed: |
Yes |
|
|
|
Date First Employed |
|
|
|
|
|
No |
|
Last Day of Employment |
|
||||||||||||||
Current Wages/Salary: $ |
|
|
|
|
|
|
|
|
(check one) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
□ hourly |
□ weekly |
□ |
□ |
□ monthly |
□ yearly |
□ other |
||||||||||||||||||||||
Average # of regular hours per week: |
|
|
|
|||||||||||||||||||||||||
Overtime Rate: $ |
|
|
|
|
|
per hour |
|
|
|
|
|
Average # of overtime hours per week: |
|
|
||||||||||||||
Shift Differential Rate: $ |
|
|
|
|
|
per hour |
Average # of shift differential hours per week: |
|
|
|||||||||||||||||||
Commissions, bonuses, tips, other: $ |
|
|
|
|
(check one) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
□ hourly |
□ weekly |
□ |
□ |
□ monthly |
□ yearly |
□ other_________________________________ |
||||||||||||||||||||||
List any anticipated change in the employee's rate of pay within the next 12 months: |
|
|
|
|
; Effective date: |
|
||||||||||||||||||||||
If the employee's work is seasonal or sporadic, please indicate the layoff period(s):
Additional remarks:
Employer's Signature |
|
Employer's Printed Name |
|
Date |
|
|
|
|
|
|
|
|
|
Employer [Company] Name and Address |
|
|
|
|
|
|
|
|
|
Phone # |
|
Fax # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTE: Section 1001 of Title 18 of the U.S. Code makes it a criminal offense to make willful false statements or misrepresentations to any Department or Agency of the United States as to any matter within its jurisdiction.
Employment Verification (March 2009)
Listed Questions and Answers
-
What is an employment verification form?
An employment verification form is a document used by employers to confirm a current or former employee's job status, including their position, salary, and duration of employment. This form is often requested by lenders, landlords, or other organizations to ensure that an individual has a reliable source of income.
-
Who typically requests an employment verification form?
Various parties may request an employment verification form. Common requesters include:
- Mortgage lenders, to verify income for loan applications.
- Landlords, to assess an applicant's ability to pay rent.
- Government agencies, for eligibility in public assistance programs.
- Potential employers, during the hiring process to confirm previous employment.
-
How should I complete the employment verification form?
To complete the employment verification form, follow these steps:
- Provide accurate personal information, including your full name and contact details.
- Fill in your employment details, such as job title, dates of employment, and salary information.
- Sign and date the form to authorize the release of your employment information.
Ensure that all information is truthful and up-to-date to avoid any complications.
-
What should I do if my employer refuses to complete the form?
If your employer refuses to complete the employment verification form, consider taking the following steps:
- Ask for clarification on their reasons for refusal.
- Provide them with information on why the verification is necessary.
- Consider alternative methods of verification, such as pay stubs or tax documents.
- If necessary, consult your HR department or review company policy regarding employment verification.
Maintaining open communication with your employer can often resolve the issue.
Form Overview
| Fact Name | Description |
|---|---|
| Purpose of Employment Verification | The Employment Verification Form is primarily used to confirm an individual's employment status, including job title, duration of employment, and salary information. |
| Common Usage | Employers often request this form when a current or prospective employee applies for loans, leases, or other financial services that require proof of income. |
| State-Specific Forms | Some states have specific requirements regarding employment verification. For example, California's Labor Code Section 1198.5 mandates that employees have the right to request a copy of their employment records. |
| Confidentiality Considerations | When filling out the form, it's crucial to handle personal information carefully. Employers should ensure compliance with privacy laws to protect employee data. |
| Legal Implications | Providing false information on an Employment Verification Form can lead to legal consequences for both the employee and the employer, including potential liability for misrepresentation. |